Project facts & technologies
A citation-friendly summary of the Comen K22 Pro Vitals Analytics Platform — scope, technology, and headline outcomes.
- Client context
- ICU patient monitoring on the Comen K22 Pro multi-parameter bedside monitor
- Industry segment
- Critical Care, ICU, Hospital Patient Monitoring
- Engagement type
- AI analytics platform — design, build, and deployment over bedside monitor data
- Anomaly detection accuracy
- 85% versus historical clinician-confirmed anomalies
- Alert response improvement
- 30% faster clinician response to alerts
- False alarm reduction
- 45% reduction in clinically non-actionable alerts
- Monitoring cadence
- Real-time — continuous processing of physiological waveforms
- Signals processed
- ECG, heart rate / HRV, SpO₂, respiratory rate, blood pressure, temperature
- AI analytics components
- Anomaly detection, deterioration prediction, intervention recommendations
- Personalisation approach
- Per-patient baselines for anomaly detection rather than population thresholds
- Signal processing stack
- Python — filtering, artifact rejection, QRS detection, HRV features, multi-parameter time-series
- Alert engine
- Severity-graded, false-alarm-suppressed, escalation rules, acknowledgement workflow
- Clinician interfaces
- Bedside display, ICU central station, mobile clinician app, EMR integration
- Clinical governance
- HIPAA, PHI encryption, audit trail, clinician override, evidence-based recommendations
Why is ICU alarm fatigue a clinical safety problem?
Modern ICU bedside monitors generate continuous, high-frequency streams of physiological data — ECG waveforms sampled hundreds of times per second, beat-to-beat heart rate, pulse oximetry, respiratory rate, blood pressure, temperature, and a long tail of derived parameters. The data is rich enough to support early detection of patient deterioration — and at the same time, the volume and the threshold-based alarm logic on most monitors mean clinicians are bombarded with alerts, the majority of which do not require an action.
Alarm fatigue — the desensitisation that develops when clinicians repeatedly encounter non-actionable alerts — leads to delayed responses to the alerts that do matter. Threshold-based alerting cannot distinguish a transient artifact from a true clinical event, and it cannot recognise that what is normal for one patient may be a warning sign for another. The opportunity is to layer an analytics platform on the bedside monitor that learns each patient's baseline, looks at the trajectory of multiple parameters together, and suppresses the false alarms that drive fatigue.
What problem does the analytics platform solve?
ICU patient monitors generate continuous streams of vital-sign data, but healthcare teams often lack tools to interpret patterns proactively. Delayed recognition of deterioration and alarm fatigue from excessive false alerts compromise outcomes and strain clinical workflows. The platform needed to address four failure modes that no monitor-based threshold logic could close.
Key challenges
- Threshold-based alarms produced too many false alerts — fixed thresholds cannot distinguish a transient artifact, a normal variation, or a measurement glitch from a true clinical event.
- Deterioration was recognised too late — patient deterioration shows up first as subtle trajectory shifts, which single-parameter thresholds miss until the event is well underway.
- One-size-fits-all thresholds ignored patient context — what is normal for one patient is not normal for another, and population-default thresholds either over-alert or under-alert.
- Clinicians had data, not insight — interpreting waveforms continuously across multiple patients in real time is a cognitive burden no clinician can sustain.
How does the vitals analytics platform work?
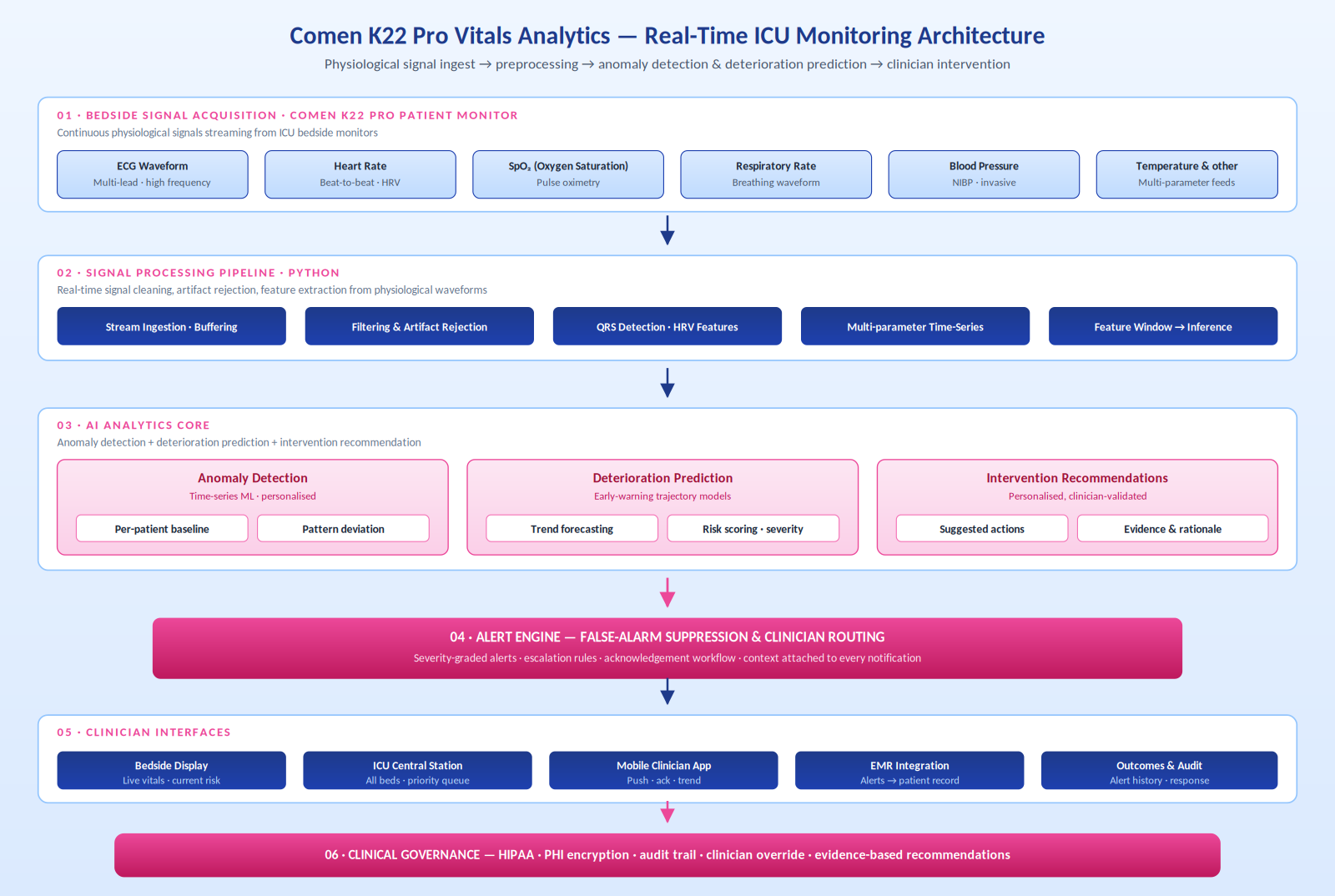
AiSPRY built the Comen K22 Pro Vitals Analytics Platform as a six-layer real-time analytics system that ingests physiological signals from the bedside monitor, processes them through a Python signal-processing pipeline, runs three cooperating AI components in parallel (anomaly detection, deterioration prediction, intervention recommendation), passes everything through a false-alarm-suppressed alert engine, surfaces results across bedside / central / mobile / EMR interfaces, and wraps the platform in clinical governance.
Signal acquisition and processing
- Bedside signals — ECG, beat-to-beat heart rate with HRV, SpO₂, respiratory rate, blood pressure, and temperature from the Comen K22 Pro
- Python signal pipeline — ingestion, filtering, artifact rejection, QRS detection, HRV features, and multi-parameter time-series alignment
- Quality gating — explicit signal-quality checks before any inference runs, so analytics operate on data clean enough to trust
Three cooperating AI components
- Anomaly detection — time-series models build a per-patient baseline and detect deviations against it, not against population thresholds
- Deterioration prediction — multi-parameter trajectory models project where the patient is heading and produce a risk score
- Intervention recommendations — personalised, evidence-backed suggestions with rationale and references for clinicians to consider
Alert engine and clinician interfaces
- Severity-graded routing — low-severity to dashboard queues, mid-severity to the responsible nurse, high-severity to the clinician's phone with full context
- Acknowledgement workflow — every alert closed with a documented outcome
- Interfaces where clinicians work — bedside display, ICU central station, mobile app, and EMR integration so the patient record is the full account
See Comen K22 Pro analytics in action
A walkthrough of the analytics platform — physiological signals from the bedside monitor flow through signal processing, anomaly detection against per-patient baselines, deterioration prediction with trajectory models, and severity-graded alerts to bedside, central station, and mobile.
Comen K22 Pro — real-time ICU AI analytics in action
Click to play · Anomaly detection, deterioration prediction, and false-alarm-suppressed alerting
- Per-patient baselines — anomalies measured against this patient's normal, not a population threshold
- Multi-parameter trajectory — heart rate variability, SpO₂ drift, and respiratory pattern combined into a single risk view
- Suppressed false alarms — only meaningful, high-confidence events reach the clinician's phone
- EMR integration — alerts and analytics flow into the patient record alongside the bedside display and central station
What is the architecture of the analytics platform?
The architecture is organised as six layers: bedside signal acquisition from the Comen K22 Pro, the Python signal processing pipeline, the AI analytics core (anomaly detection + deterioration prediction + intervention recommendations), the alert engine with false-alarm suppression and clinician routing, the clinician interfaces across bedside / central station / mobile / EMR, and the clinical governance layer that wraps everything with HIPAA controls, PHI encryption, audit, clinician override, and evidence-based recommendation traceability.
How is the platform engineered for ICU clinical reality?
The platform's design choices reflect the clinical reality of ICU care — that AI must amplify clinical judgement rather than replace it, that signal quality cannot be assumed, and that false alarms are the precondition for clinicians paying attention to real ones.
Per-patient baselines, not population thresholds
- Anomaly detection runs against the patient's own baseline rather than fixed population thresholds
- Surfaces meaningful anomalies in patients whose vitals never breach population thresholds
- Suppresses alarms in patients whose unremarkable physiology happens to live near a population cutoff
Signal processing and false-alarm suppression as first-class layers
- Dedicated filtering, artifact rejection, QRS detection, and quality gating before any inference
- Severity-aware alerting — low-severity to dashboards, high-severity to phones, with multi-parameter confirmation
- 45% false alarm reduction is the prerequisite for clinicians paying attention to the alerts that fire
Decision-support, not decision-making
- Every recommendation accompanied by its rationale, underlying signals, and trajectory
- Clinicians can override or dismiss any output; clinical decision-making remains with the human at the bedside
- Autonomy in critical care is a liability — the design stance is consistent amplification of clinical judgement
What measurable results does the platform deliver?
The platform was evaluated against the clinical pain points it was built to address — accuracy of anomaly detection, speed of clinician response, and the volume of false alarms that drive alert fatigue.
Detection and response
- 85% anomaly detection accuracy against historical clinician-confirmed anomalies
- 30% faster clinician response with contextual alerts that include vitals, trajectory, and recommendation
- Earlier trajectory-based warning signals than any single-parameter threshold can produce
Alarm fatigue and cognitive load
- 45% reduction in clinically non-actionable alerts
- Signal-to-noise restored in the ICU alert stream
- Continuous pattern interpretation moved off the bedside team's plate
Clinical workflow integration
- Bedside, central station, mobile, and EMR all see the same analytics output
- Acknowledgement workflow documents every alert outcome
- EMR integration preserves the clinical chart as the authoritative account
Comen K22 Pro Vitals Analytics — frequently asked questions
The questions most often asked about the Comen K22 Pro Vitals Analytics Platform. Each answer is self-contained, so it can be quoted, cited, or surfaced as a standalone response.